** This is an ongoing case. I am in the process of updating and editing this ELOG as and when required.
Note: This is an online E Log book recorded to discuss and comprehend our patient's de-identified health data shared, AFTER taking his/her/guardian's signed informed consent.
Here, in this series of blogs, we discuss our various patients' problems through series of inputs from available global online community of experts with an aim to solve those patients' clinical problems, with collective current best evidence based inputs.
This E-log book also reflects my patient-centered online learning portfolio and of course, your valuable inputs and feedbacks are most welcome through the comments box provided at the very end.
I have been given the following case to solve, in an attempt to understand the concept of "Patient clinical analysis data" to develop my own competence in reading and comprehending clinical data, including Clinical history, Clinical findings, Investigations and come up with the most compatible diagnosis and treatment plan tailored exclusively for the patient in question.
CASE SHEET
Chief complaint: Multiple bouts of vomiting and inability to hold down any water since episode of binge drinking. Patient also missed an Insulin dose on the night of drinking
History of presenting illness: Patient was asymptomatic 2 days ago
He had an episode of bimge drinking on the 5th of September after which he went home and slept
On that night he missed his dose of Insulin.
On 6th September Patient could not hold down any liquid consumed and kept vomiting anything he consumed.
He was taken to a private practice after which his blood sugar was measured and reported to be 600mg/dl.
He was given medication (insulin, antiemetic? ) and his vomiting episodes reduced
On the morning of 7th September he was brought to our ICU and has been undergoing treatment for Diabetic Ketoacidosis
He was diagnosed with Diabetes 2 years back on visiting a physician pertaining the complains of polydypsia and polyuria
Patient has made no lifestyle modifications following diagnosis. However takes medication regularly
History of past illness:
Known case of diabetes since 2 years
No history of hypertension, asthma, Tuberculosis or seizures
Drug history: Patient has been taking a combination of metformin hydrochloride and Insulin 15U(BD) for type 1 diabetes mellitus.
Personal history:
Mixed normal appetite till before current episode of DKA
Normal bowel movement
Normal micturition
No known allergies
Chronic smoker. Patient doesn't recall when he started smoking. Currently smokes 2 to 3 cigarettes per day
Consumes Alcohol once in every 4 to 5 days. Approx 200 to 300ml
Family history: Father is known case if diabetes
General examination:
Pallor: Absent
Icterus: Absent
Cyanosis: Absent
Clubbing: Absent
Koilonychia: Absent
Lymphadenopathy: Absent
Edema: Absent
Vitals:
Temperature: 99
Respiratory rate: 45 breaths per minute
Pulse : 120 beats per minute
Blood pressure: 100/70 mm of Hg
CVS examination:
Respiratory system examination:
.
CNS examination:
Higher functions:
Speech:
Gait
Cranial nerves:
Blood sugar
Hemogram:
Urine analysis:
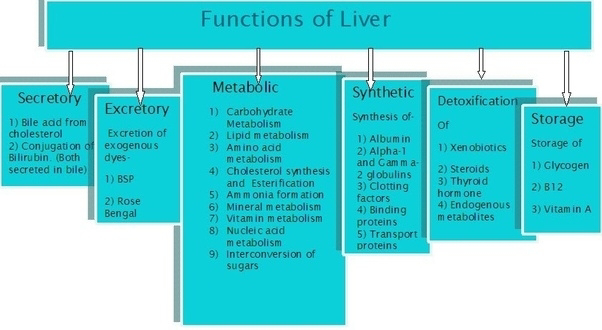
LFT
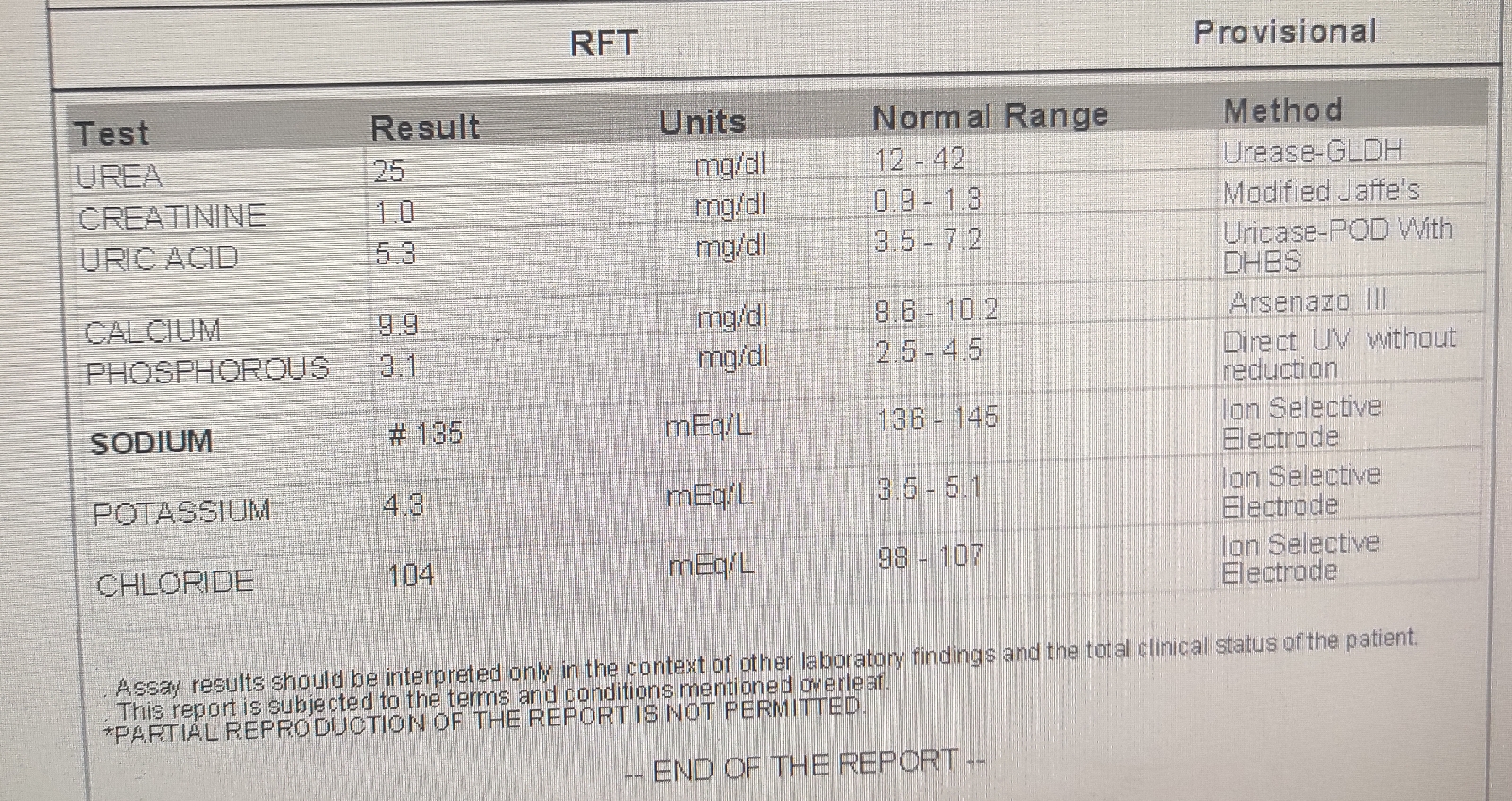
RFT
BLOOD UREA
Creatinine
ECG
Provisional Diagnosis: Diabetic Ketoacidosis
Treatment:
Day1
Infusion normal saline @125ml/hour
Injection Human Insulin 6U IV stat
H. A insulin 6ml/hr IV initially. Now on 2ml/hr IV
Injection Pantop 40mg IV/UD/BBF
Injection Zofer 4mg IV/BD
GRBS monitoring every hour



















Comments
Post a Comment